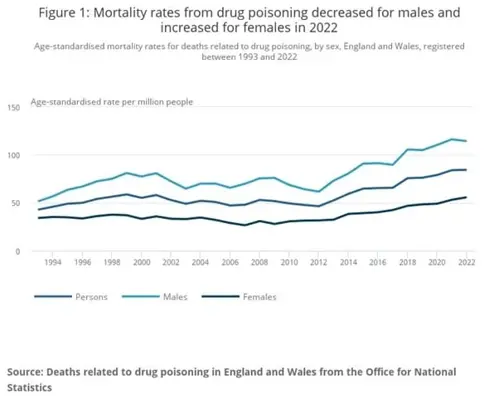
In 2022, 4097 people died in England and Wales from drug poisoning (ONS). 2261 of the deaths involved an opiate.
Table from ONS
In 2021, the government set a target, as part of “From harm to hope: A 10-year drugs plan to cut crime and save lives” to prevent nearly 1,000 drug related deaths by the end of 2024 to 2025.
Naloxone was patented in 1961 and can reverse the effects of an opiate overdose – but only if given before hypoxia due to reduced respiration has done irreparable harm.
We have the ability to treat opiate overdose with naloxone and oxygen – but it seems that the need to administer the antidote quickly isn’t appreciated by the national bodies who could make a difference, save lives and help the government hit at least one of their targets.
NHS Pathways is an algorithm used by ambulance service call handlers to triage 999 calls, and to advise the call handler about what should be done for the caller. Call handlers are not clinicians (starting salary £23,000 per annum).
Some of these calls result in the dispatch of an ambulance – the category of the ambulance is suggested by the algorithm.
Category 1 is for calls about people with life-threatening injuries and illnesses – average time from 999 call to the correct person arriving should be 7 minutes.
Category 2 is for emergency calls – 18 minutes
Category 3 is for urgent calls – 9 out of 10 times the response will be within 120 minutes.
Given that opiates can cause death by overdose in minutes, you might expect that a 999 call reporting a fentanyl overdose would elicit a rapid response to deliver paramedics, naloxone, oxygen and an oximeter to the patient.
Not so – the NHS pathway will send a category 3 ambulance if the patient is alert and breathing after a fentanyl overdose at the time of the 999 call. That’s a 90% chance the ambulance will arrive within 2 hours.
In November 2023 a coroner sent a Regulation 28 Prevention of Future Deaths report to NHS England who manage the NHS Pathway about this issue. The report raised the concern that the current NHS Pathways process does not differentiate between a high risk and low risk overdose, categorising all such calls without additional symptoms as Category 3.
The NHS England response was -
“Where an overdose has occurred, and in the absence of signs or symptoms indicating an immediate life-threat (reduced conscious level, breathlessness, or shock, for example), the lowest disposition that can be reached is a Category 3 ambulance response. A quicker response will be actioned where there are symptoms indicating an immediate life threat. In April 2021, NHS England and Improvement, in collaboration with the Association of Ambulance Chief Executives (AACE) published a new operational procedure for all ambulance services in England which sets out that, where an overdose is declared, a further clinical intervention should take place within 30 minutes, and/or the case will be automatically upgraded to a Category 2 ambulance response if this does not occur within 40 minutes”
If the caller says they’ve taken an overdose, it could be 30 minutes until someone who understands the situation will make a decision - by which time the patient may well be beyond treatment.
The response from NHS England also states
“Governance of NHS Pathways. The safety of the clinical triage process endpoints resulting from a 111 or 999 assessment using NHS Pathways, is overseen by the National Clinical Assurance Group (NCAG), an independent intercollegiate group hosted by the Academy of Medical Royal Colleges. This group is made up of representatives from Medical Royal Colleges and other clinical professional bodies and groups. Senior clinicians from these organisations provide independent oversight and scrutiny of the NHS Pathways clinical content. The group considers all aspects of the triage process, including the impact on services, as well as the evidence base for changes to the clinical content.”
I can’t find out who the people on NCAG are, so I don’t know if any of them are qualified to consider the treatment of opiate overdose.
The response does not say that there is any process for informing NCAG of Prevention of Death Notices, which seems unfortunate as it seems to be their responsibility to balance risk, benefit and cost.
The response doesn’t mention naloxone, and doesn’t indicate that change is planned.
In the early 80s I was a junior doctor in A&E when a young woman presented after a coproxamol overdose. She gave me her story and I stepped out of her cubicle for a few minutes to collect blood sample tubes and answer my bleep. When I returned, she was blue and unresponsive. Luck, naloxone and an ambu bag with oxygen rescued her.
Forty years later, my sister-in-law called 999 to report that my brother had swallowed his prescribed fentanyl patch but was still conscious. It’s clear from the transcript of the 999 call that the call handler had no idea what fentanyl was. A category 3 ambulance was selected as NHS Pathways dictated. The police arrived 45 minutes after the 999 call, and found him collapsed. In that area the police don’t carry naloxone. The police gave CPR when he arrested about 15 minutes after they arrived. The ambulance service attended 64 minutes after the initial 999 call – the police had requested a category 1 ambulance which arrived 13 minutes after their call.
Had a category 2 ambulance been dispatched after the initial 999 call and arrived by 18 minutes, the naloxone might have been effective, and the coroner would not have been involved.
As my brother would have said – computer says no!
Dr Diane Ackerley
Certificate in the Management of Drug Misuse October 2002
References
Other News & Events